




Listen to this article
Medical affairs leaders aren’t struggling with a lack of evidence. They’re struggling with how that evidence lives.
What your teams generate, curate, and synthesise is scattered across systems, and takes too long to come together, making it hard to drive decisions at the pace the business now expects.
ntegrated Evidence Planning (IEP) was designed to solve exactly this. And yet for most organisations, IEP remains a point-in-time exercise, a plan built at the start of a cycle that's partially outdated before it's even approved. The frameworks are there. The intent is right. The gap is in the infrastructure that keeps an evidence strategy alive between planning cycles.
This is the gap that creates HTA surprises, which makes cross-market alignment feel like negotiation rather than alignment. This, in turn, converts pre-submission periods into evidence chases rather than evidence strategy.
The context your IEP wasn't built for
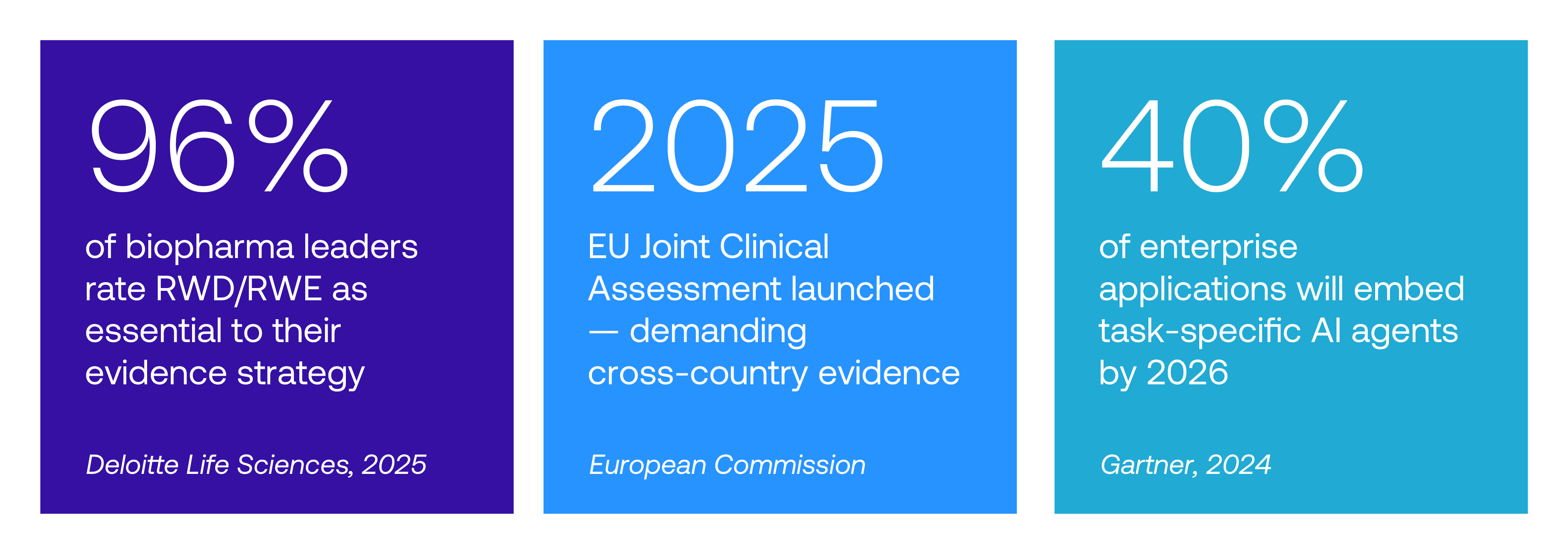
The expectations placed on medical affairs evidence have structurally shifted in the last three years, and the planning infrastructure at most organisations hasn't kept pace.
Europe's Joint Clinical Assessment, which came into force in 2025, demands cross-country consistency in a way that exposes any gap between how markets have independently interpreted the evidence base. NICE and IQWiG have both sharpened their guidance on RWE methodology. The bar for bias mitigation, provenance, and external validity has moved up. Payers are increasingly using real-world data to re-examine launch-era decisions, meaning an evidence strategy that was sufficient at approval may not be sufficient at reassessment.
None of this is new information to medical affairs leaders. What's underappreciated is the demand of your planning infrastructure, not just the quality of individual studies, along with the ability to hold a coherent, current, and comparable evidence story across markets, data types, and time.
Where the evidence strategy breaks down
The failure mode isn't usually a single gap in the evidence base. Two patterns appear repeatedly.
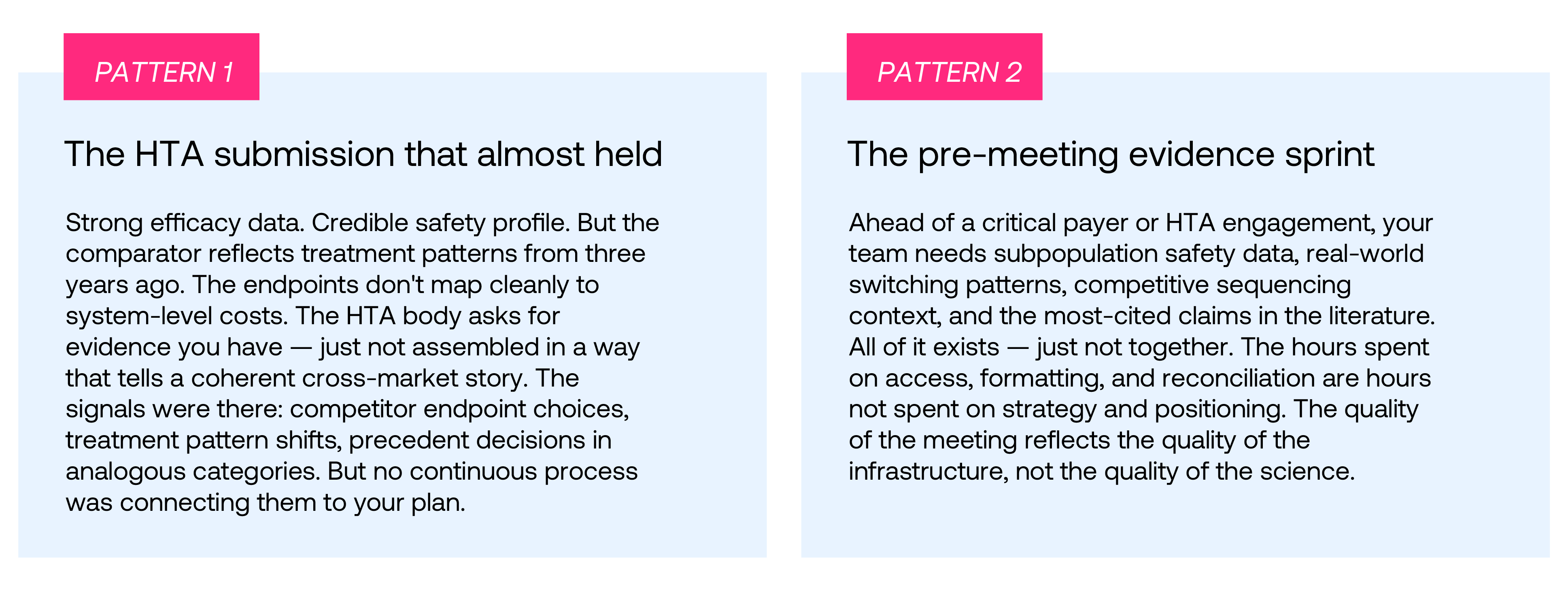
“The hours spent on access, formatting, and reconciliation are hours not spent on strategy. The quality of the meeting reflects the quality of the infrastructure, not the quality of the science.”
Both patterns share the same root cause: an evidence strategy that exists as a document rather than as a living system. One that was built for a planning cycle rather than for the pace at which the evidence landscape moves.
What this means for medical affairs leadership

From evidence planning to evidence intelligence
The step-change isn't in building a better IEP template. It's in shifting from a planning artefact to a continuously updated intelligence layer, one that connects your clinical data, real-world evidence, safety signals, publications, and competitive landscape into a single, coherent view.
Evidence AI Analyst, powered by Flow AI, is built for exactly that. It's not a search tool. It's not a dashboard. It's an AI layer that sits across your evidence corpus and does the connective work that currently falls to your most experienced people.
- Synthesis across data types — Clinical trials, RWE, regulatory documents, safety data, and publications read together, returning explainable answers with full source lineage. The kind of synthesis that currently takes a team days to assemble manually.
- Proactive gap detection — Emerging evidence gaps, competitor portfolio moves, and HTA precedent shifts surfaced before they become submission problems. Surprises become scenarios you already modelled.
- Continuous cross-market consistency — A shared, comparable evidence foundation maintained across markets as a living standard, not rebuilt market by market ahead of each engagement.
- Strategy re-threading in real time — When a competitor pivots or new science appears, the implications for your evidence plan surface immediately. Not at the next planning cycle.
The medical affairs leaders who will be best positioned for the 2026 evidence environment aren't the ones with more data. They're the ones whose evidence strategy is connected, current, and ready to defend, not as a document produced at planning time, but as a living system that moves with the science. That's the shift Evidence AI Analyst is built to enable.
Evidence AI Analyst · Powered by Visionet AgentVerse platform
What does continuous evidence intelligence look like for your team?
See how medical affairs leaders are shifting from point-in-time planning to a living evidence strategy, connected inputs, explainable outputs, and submissions built on a foundation that doesn't need to be rebuilt from scratch each cycle.
